






Remember the days of the Miller Light commercials with various ex-athletes screaming “Less Filling” versus “Tastes Great” at each other. Academic researchers in nutrition are no different. The latest example of this was a recent article in Cell Metabolism in which the authors state that their carefully controlled study demonstrates that you lose more fat on a low-fat diet than a low-carb diet (1). That’s like waving a red flag in the face of a raging bull (i.e., the groups of academics claiming it is impossible to lose fat without lowering insulin).
As with politics and Hollywood, you usually have to go behind the scenes to get the real facts. Let’s first start with the Cell Metabolism study. There is the gold standard for measuring body fat. It is known as a DXA analysis. This is the most precise and reproducible method known in obesity research. In Table 3 of the Cellular Metabolism article, both groups lost about 1 pound of fat on either diet, but there were no statistical differences between the two groups. Yet the title of the paper is “Calorie for calorie, dietary fat restriction results in more body fat loss than carbohydrate restriction in people with obesity”. So how do the authors explain this apparent lack of correlation of the title of the paper with their own data? They state, “We suspect that DXA measurements of fat-mass change in the present study were insufficiently sensitive to detect differences between the diets”.
Maybe the reason was because there were no real differences in fat loss between the two diets. Nonetheless, they then come up with some complex mathematical measurement based on fat intake and net fat oxidation minus de novo lipogenesis measured by indirect calorimetry (a technique that could never be replicated by anyone else without using the same metabolic chamber) to finally get a number that supports the title of the article. This sounds like medieval theologians describing a technology for determining the number of angels that can stand on the head of a pin.
Let’s go back again to Table 3 in the Cellular Metabolism article, and you find that those on the reduced-carbohydrate diet lost more weight than those on the reduced-fat diet; and that difference was statistically significant. Although I agree with the author’s statement, “Fat loss is more important than weight loss in the treatment of obesity”, actually what is medically important in the treatment of obesity is the ability of a diet to reduce inflammation and insulin resistance and simultaneously increase satiety. According to Table 4 the same Cellular Metabolism article, there were no differences between the two diets in reducing inflammation or insulin resistance as well as no measurement of reduction of satiety. This would indicate that the study was pretty worthless.
Despite these pathetic clinical results, an accompanying editorial paper praised the study as “one strike against low-carbohydrate diets” (2). I found that remark interesting since that same author was also an author of a 1999 article in Pediatrics that demonstrated dramatic changes in hormones and lack of hunger in obese children after eating a single Zone meal compared to eating isocaloric meals with higher-carbohydrate contents (3). I guess she forgot her part in that earlier-published research.
So why was the data so meaningless in this highly touted article? I believe because the study was poorly designed. First is you can’t treat obese males and females as identical. The average lean-body mass of the males in the study was 162 pounds and that of the females was 120 pounds. Based on my books The Zone and Mastering the Zone (both were New York Times best sellers and each book sold more than one million copies each), an obese, sedentary person would need 0.7 grams of protein for each pound of lean body mass to maintain their muscle mass (4,5). This means the males should have consumed 113 grams of protein per day and the females 84 grams of protein per day to maintain their muscle mass.
So let’s compare my Zone Diet recommendations for these same obese male subjects versus what they actually got in this study as shown in Table 1. I am only focusing on the males for later comparison in this blog to earlier studies that also used only males.
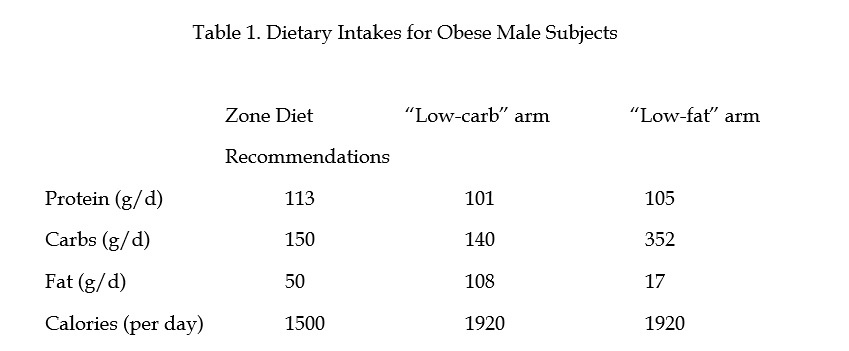
In the weight loss phase of the study, the males in this study were protein-deficient. According to my books, once you determine the protein level in the diet to prevent loss of muscle mass, then that automatically determines the levels of carbohydrates, fat, and total calories in the rest of the diet. Furthermore, to make Table 1 simple to understand, remember that the Zone Diet is essentially a 1:2:3 ratio of fat-protein-carbohydrate. That means the Zone Diet is a balanced diet as opposed to the two highly unbalanced diets used in this study.
From Table 1 you can see that in the “low-carb” arm of the study, the levels of protein and carbohydrates are almost identical to the levels recommended by the Zone Diet (and dietary guidelines of the Joslin Diabetes Research Foundation for treating metabolic syndrome and type 2 diabetes (6)). However, the obese males in the study were consuming more than double the amount of recommended dietary fat following the Zone Diet (as well as the Joslin dietary guidelines) in the “low-carb” arm. On the other hand, the “low-fat” arm had Dean Ornish-like levels of fat and excessive levels carbohydrates. Therefore both of the experimental diets used in the study were extremely unbalanced compared to the Zone Diet. Furthermore, the subjects were also consuming more than 400 calories each day on their “weight-loss” diet compared to my recommendations of the Zone Diet (as well as the Joslin dietary guidelines).
Maybe the Zone Diet recommendations (as well as those from the Joslin Diabetes Center) are too difficult to follow?
Unfortunately, the authors of this new study overlooked a major study published in the American Journal of Clinical Nutrition in 2000 by Harvard researchers that actually had very different results (7).
In this Harvard study, the researchers did the same randomized, crossover study as used in the Cell Metabolism study, but they used only overweight and obese males (average BMI of 31). For the first two days of this earlier study, the subjects were allowed to eat whatever they wanted in a metabolic ward. For the next six days they had to consume the test diets made for them. Then in the final two days, they got the same test diets but had access to a private food buffet in their metabolic ward if they wanted more food. Fortunately, the lead author knew something about the Zone Diet, so one of the two arms of this study was essentially the Zone Diet versus an isocaloric diet with higher carbs but lower levels of protein and fat. Both arms contained 1,500 calories (pretty much what the Zone Diet recommends) for sedentary obese males with three identical meals of 450 calories each and late-night snack of 150 calories as I usually recommend (4,5). However the macronutrient levels the different diets were very distinct as shown in Table 2.
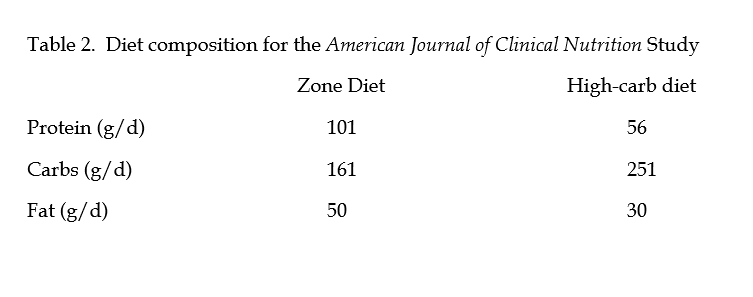
It should be noted that Zone Diet group was consuming essentially the same amounts of protein and carbohydrates as the “low-carb” arm of the Cell Metabolism study but without the massive amount of extra fat.
Now what about the results? Like the Cell Metabolism study, the weight loss in both groups was the same. Like the Cell Metabolism study, the Zone Diet had lower insulin responses. However, the subjects in the American Journal of Clinical Nutrition study lost far more weight than in the Cell Metabolism study. This means if you want to lose weight, you have to reduce calorie intake. Another key factor in the American Journal of Clinical Nutrition study was the subjects consuming the Zone Diet consumed 25% fewer calories from the open buffet on two days they had access to it compared to when they were consuming the high-carbohydrate diet. This means they weren’t as hungry following the Zone Diet. If you aren’t hungry, then you can stay on a calorie-restricted diet for a long time.
In addition, those on the Zone Diet were not losing muscle mass since they had a positive nitrogen balance, whereas when they were consuming the high-carb diet they were losing muscle mass. Finally, the reduction in their resting energy expenditure following the Zone Diet was more than 50% less compared to when they were following the high-carbohydrate diet. This means that their bodies were not undergoing a starvation response usually seen with calorie-restricted diets.
The Harvard researchers repeated the same type of study with the same diet composition with younger obese male individuals in 2004, but now they used a parallel group study as opposed to a crossover study. Once again there were no differences in the weight loss or even the fat loss of either group when they followed their respective calorie-restricted diets (8). However, those subjects following the Zone Diet more than doubled the decrease in insulin resistance and had a 9 times greater reduction in C-reactive protein than the subjects in the high-carbohydrate diet group. That is what a medically useful diet is supposed to do.
So what does this all mean? First, the statement that a “calorie is a calorie” is probably true relative to weight loss and fat loss. To lose weight or body fat, you have to cut calories. It also means to maintain that initial weight or body-fat loss, you probably have to restrict your calories forever (9). This also explains why weight loss is easier than weight maintenance (10). Second, the same statement that a “calorie is calorie” is not true relative to hormonal changes, insulin resistance and inflammation and reduction of hunger. This means to maintain a calorie-restricted diet without hunger and to generate the positive health benefits of weight loss is highly dependent on the macronutrient balance of the diet. The most successful diet to achieve both goals remains the Zone Diet.
Here lies the problem with high-anything diets—they will never work. If you are stuffing excess fat into a diet (even a calorie-restricted diet), that excess fat ends up in the bloodstream. The body will oxidize that incoming dietary fat first before releasing the stored fat from the adipose tissue even if insulin levels are reduced. On the other hand, if the fat levels in the diet are low, but the carbohydrate levels are high, then the excess insulin produced by that unbalanced diet will make it very difficult to release excess stored fat in the adipose tissue forcing the body to begin to cannibalize its muscle mass for needed energy as evidenced by going into negative nitrogen balance and reduction in resting energy expenditure. Since the body switches between carbs and fat for energy, the key for any long-term diet success means maintaining adequate protein to increase satiety (this is why the subjects in the Harvard study ate less food) and maintain muscle mass while decreasing the amount of the other incoming macronutrients (carbs and fat) that are easily converted into energy, thus encouraging the adipose tissue to release stored fat.
This has always been the story of the Zone Diet. It is a protein-adequate, low-carb and low-fat diet that increases satiety and reduces inflammation. Since my two New York Times best sellers (although they were published in the 20th century) describe this approach in highly practical and readable detail, you would think more academics would have read them. Maybe in this century my books on the Zone Diet may be rediscovered. Until that time, we can expect more academic food fights.
References:
- 1. Hall KD et al. “Calorie for calorie, dietary fat restriction results in more body fat loss than carbohydrate restriction in people with obesity.” Cell Metabolism 22: 2-22 (2015).
- Roberts SB and Das SK. “One strike against low-carbohydrate diets.” Cell Metabolism 22:1 (2015).
- Ludwig DS et al. “High-glycemic-index foods, overeating, and obesity.” Pediatrics 103:e26 (1999).
- Sears B. The Zone. Regan Books. New York, NY. (1995).
- Sears B. Mastering the Zone. Regan Books. New York, NY (1997).
- Joslin Diabetes Center and Joslin Clinic. “Clinical nutritional guideline for overweight and obese adults with type 2 diabetes, prediabetes or those at high risk for developing type 2 diabetes.” (2007).
- Agus SD et al. “Dietary composition and physiological adaptations to energy restriction.” Am J Clin Nutr 71:901-907 (2000).
- Pereira MA et al. “Effects of a low-glycemic-load diet on resting energy expenditure and heart disease risk factors during weight loss.” JAMA 292:2482-2490 (2004).
- Klem ML et al. “A descriptive study of individuals successful at long-term maintenance of substantial weight loss.” Amer J Clin Nutr 66:239-246 (1997).
- Fildes A et al. “Probability of an obese person attaining normal body weight.” Amer J Public Health 105:e54-59 (2015).

Let Us Know What You Thought about this Post.
Put your Comment Below.